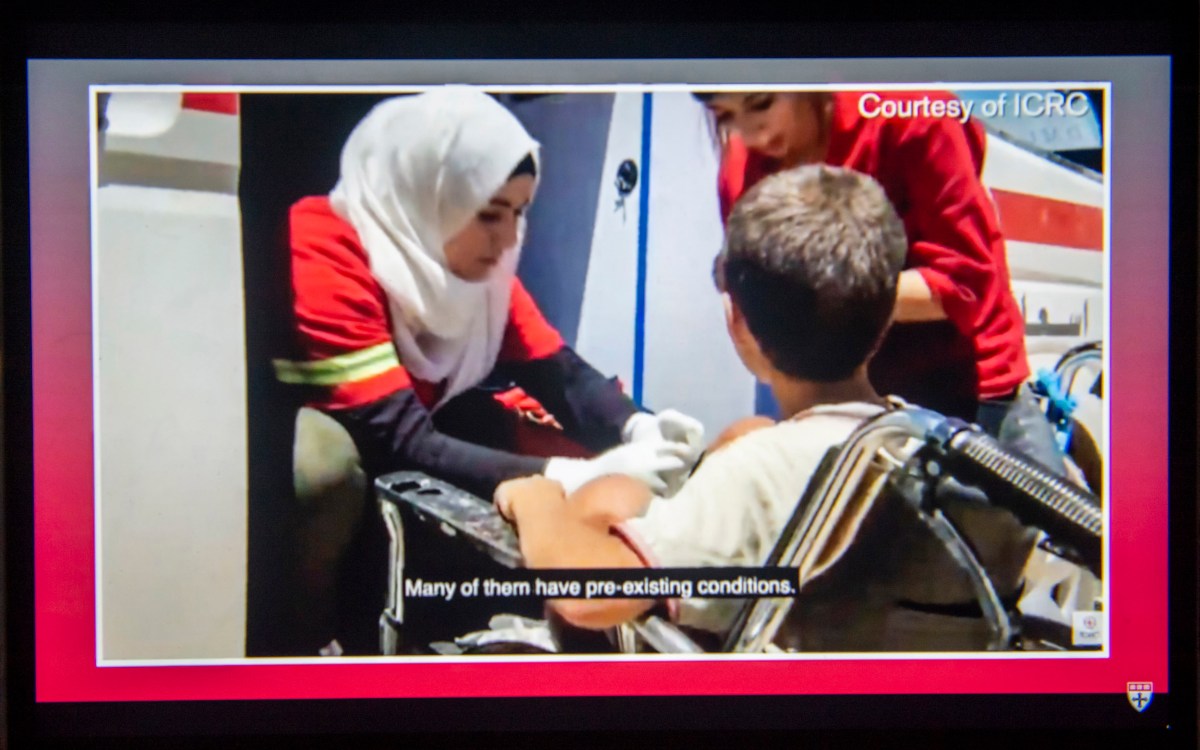
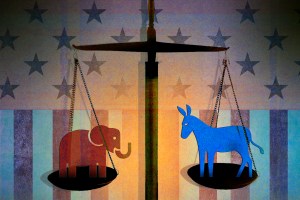

Morgan Broccoli tends to a patient in Haiti after the country was hit by a 7.2-magnitude earthquake in 2021.
Photos courtesy of Morgan Broccoli
Nation & World
A doctor’s lessons from Haiti, Turkey, Ukraine border
Rushing to war and disaster zones to provide urgent care has convinced Morgan Broccoli there’s a smarter way to help
When Harvard physician Morgan Broccoli landed in Turkey in February, she noted two things. The first was the sheer scale of devastation caused by the Feb. 6 earthquakes in Turkey and Syria, which killed more than 50,000, injured more than 112,0000, and left more than 1.5 million homeless and in need of humanitarian assistance. The second was the enormity of the search-and-rescue process underway.
“There were so many teams from all over the world going through these collapsed buildings — it was amazing to see.”
Transformative trip
Broccoli did not originally intend to go into disaster and humanitarian work. An emergency doctor and clinical fellow at Brigham and Women’s Hospital and Harvard Medical School, most of her work had focused on healthcare systems strengthening and education. That is, until 2021, when she was offered a place on a trip to Haiti with Team Rubicon, a nonprofit disaster relief organization.
Haiti had been hit with a double disaster within two days: a 7.2 magnitude earthquake and then a direct hit from Tropical Depression Grace, which triggered a series of devastating mudslides. With more than 2,200 killed and tens of thousands of buildings destroyed, it was 2021’s worst natural disaster — and for a country already reeling from the assassination of its president and an explosion of gang violence, a dire escalation of an already-critical humanitarian situation.
Broccoli deployed to Les Cayes, close to the epicenter, to join a team of local doctors and emergency personnel. “As part of this recon team, I had the chance to be one of the first physicians out the door, helping set up systems and responses alongside local healthcare programs,” Broccoli said. Their first task was to provide acute medical care to people in the earthquake zone, such as setting broken bones and cleaning wounds. Broccoli and her team worked closely with local physicians, nurses, and other partners, whom she calls “completely invaluable.”
The situation inspired her to begin thinking systematically about how best to support countries with a low capacity for disaster response, like Haiti.

Emerging from disasters stronger
“We call it resilience — this idea that the state can respond to its own disasters internally, without requiring much help from outside organizations,” Broccoli said. “That’s the ideal state. In the global medicine space, we are essentially always trying to build ourselves out of a job. Of course, it’s not always possible, as there are differing degrees of disasters — but that’s the goal.”
In February 2022, she traveled to Poland to assess the needs of the first wave of refugees from Ukraine, giving her a firsthand view of a different sort of crisis.
“It’s hard to compare the conflict in Ukraine to a natural disaster,” she said, “as conflict settings have their own set of unique challenges. And as the Ukraine war has turned into a protracted crisis, these challenges have evolved.” In addition to continued conflict-related injuries and psychological distress, people now also struggle with subacute medical needs: “For example, even here in the U.S. there are many patients with uncontrolled hypertension because they have trouble accessing primary care — these kinds of things become even more difficult in a conflict setting.”

Earlier this year in Turkey, Broccoli worked once again to embed herself with local teams. Unlike some of the other places she’d visited, Turkey had robust and high-functioning healthcare and disaster response mechanisms in place; the region had simply been overwhelmed by the enormity of the crisis.
“The earthquake just devastated healthcare infrastructure in Turkey,” Broccoli said. “So many people died — and on top of that, the people in the area now had nowhere to sleep, no shelter, and it was so cold. Many hospitals had completely collapsed.”
Across the border in Syria, these challenges were exacerbated by the ongoing civil war, which had already led to high levels of displacement and vulnerability and made getting aid into the country difficult.
“Everyone knew that although Turkey was the epicenter, the instability and war in Syria would create a lot of challenges in terms of disaster response,” said Broccoli. She and colleagues ultimately were unable to enter the country due to logistical issues. However, she noted that the World Health Organization has been working to overcome these hurdles to get foreign medical teams into the country, and that “many health organizations have already become established in this area over the past 10 years, so our focus will be on how we can help those organizations function as best they can.”
Before the next crisis
At the time of this interview, Broccoli was in Zambia, working to implement a package of emergency care tools, such as online courses and trauma care checklists, and track outcomes. Having worked with a nonprofit that does emergency care work across Africa in medical school, she said, “this is where I got started and, really, where my heart is.”
“In the global medicine space, we are essentially always trying to build ourselves out of a job.”
She’s also developing online courses in emergency medicine that can be easily implemented across different humanitarian settings. Following her trip to Poland, she partnered with the Harvard Humanitarian Initiative and Brigham and Women’s, Massachusetts General, and Boston Children’s hospitals to create a series of online courses on mass casualty management, including lessons in hands-on clinical care, how to build hospitals from the ground up, and disaster planning for use in Ukraine and other settings. She also advises countries on developing national healthcare packages with humanitarian considerations in mind and teaching hospitals how to develop mass casualty plans. Education and systems strengthening, it turns out, are key to improving disaster and humanitarian response capabilities.
In addition to her work at Brigham & Women’s and consulting for the World Health Organization, she continues to look for opportunities to join recon teams — both to better understand the unique challenges faced in different types of humanitarian crises and to help those struggling in their wake. “I’ve found that as some of the first people in, we can make a really meaningful impact.”